Introduction
Parkinson's disease (PD) is associated with many putative environmental (1) and genetic (2) risk factors which in combination result in heterogeneity of onset symptoms, blend of motor and non-motor clinical features, and rate of disease progression. This disease heterogeneity has been recognized as a major challenge for disease modifying research because addressing mechanistic processes involved in one subtype would not be expected to slow progression of a different subtype. For example, some PD patients develop early dyskinesias and motor fluctuations suggesting acceleration of pathology in the nigral dopaminergic pathways while others develop early progression of gait difficulty and cognitive decline implying early spread of the alpha-synucleinopathy into the cerebral cortex. Accordingly, one of the highest priorities for clinical research identified by the National Institute for Neurological Disorders and Stroke (NINDS) Parkinson's 2014 Conference was to “characterize the long-term progression of PD and understand the mechanisms that underlie the heterogeneity in clinical presentation and rates of progression” (3). Moreover, the study of drugs aimed at slowing progression is limited by the practical need to organize clinical trials that can be completed in a reasonable time frame of < 5 years. The problem is that on average, PD progresses slowly with a median survival time of 15.8 years (4). Though the long range goal in pursuit of precision medicine is to design trials in well-defined, homogeneous biological subtypes, this will only be possible with future identification of robust prodromal biomarkers (5). In the meantime, being able to predict in early disease the likelihood that a given individual will progress rapidly could be useful for enriching disease modifying clinical trials with fast progressors.
Results
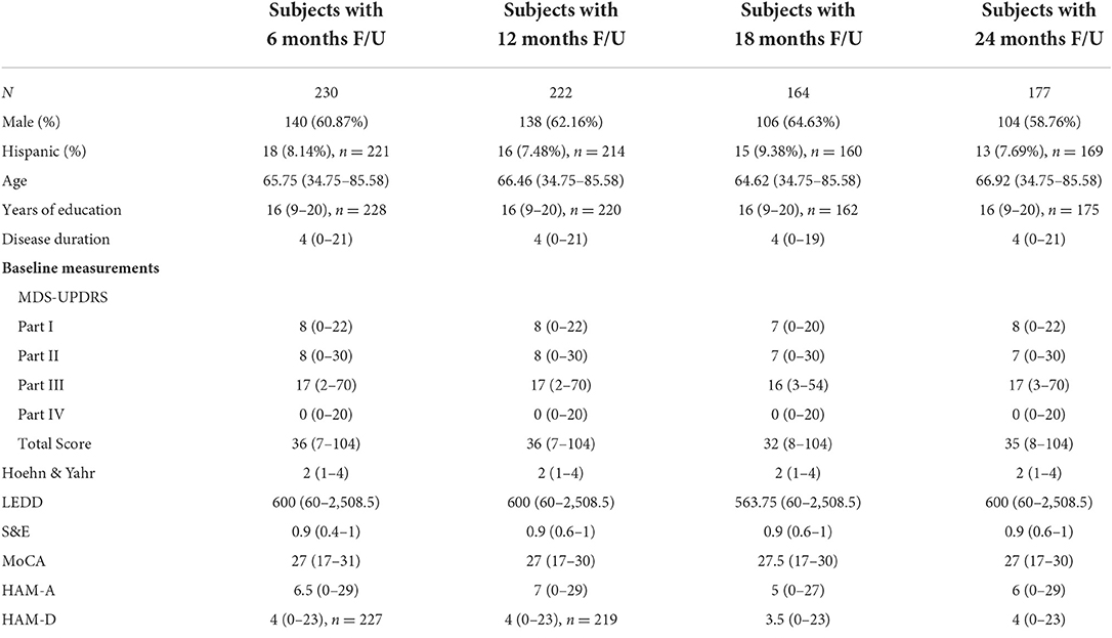
Baseline clinical scores and demographic information were available for 230, 222, 164, and 177 PD subjects in the four follow-up groups as shown in Table 1. The groups were very similar with respect to clinical features. Table 2 shows the median change (in units per year) for the groups classified by duration of follow-up. Note that no significant change was seen at 6 and 12 months of follow-up in any clinical measure. By contrast, after 18 months of follow-up the MDS-UPDRS total score had increased by a median of 3 points with a 90 mg/day increase in LEDD. Further progression in all clinical measures was noted by 24 months of follow-up. The accuracy of APDM gait and balance measures at baseline for predicting future change in clinical outcomes is shown in Table 3. The results are poor out of sample accuracy for all time points except for modest prediction of progression at the 6-month follow-up visit. Of note, there was no actual change in the two clinical variables available at the 6-month time point.